![]()
State of Knowledge
Helmut Walter
In the Eighties T. Karu began to search for the photobiological "recipient" on cells level. In a series of publications (which were combined in a book) she was able to proof, that respiratory enzymes of mitochondrias are the main photo - acceptors.
The Stimulation of the Respiratory Chain
 Fig. 1: Human metabolism
Fig. 1: Human metabolism
To understand exactly, where the laser radiation intervenes,
the facts of the respiratory chain will be explained shortly:
The respiratory chain, also called electron transport chain or oxidative
phosphorolysis, is the last step in human metabolism: The complex metabolits
of our daily food, such as carbohydrats, lipids and proteins are first
catabolized to their monomer units, especially glucose, fatty acids, glycerin
and aminoacids and then to their common intermediate product acetylcoenzyme A
(Acetyl-CoA). In the tricarboxylic acid cycle (TCA cycle) acetylcoenzyme A is
oxidated with O2 to CO2. At the same time the coenzymes
NAD+ and FAD are reduced to their energy rich intermediate products
NADH and FADH2. In the last part of this metabolism, called
transport of electrons or oxidative phophorylation, these energy rich
intermediate products are re-oxidated, that is electrons are transfered from
NADH or FADH2 to the oxygen, which therefore is reduced with two
additional protons to H2O. The released energy stimulates the
synthesis of energy rich ATP out of ADP via phosphorolysis with Pi. (fig.1)
While glycolysis happens in the cytosol of the cell, the oxidative metabolism (tricarboxylic acid cycle, oxidation of fatty acids and transport of electrons and oxidative phosphorylation) happens in the mitochondria. These are spherical to rod-shaped, membrane-bounded cytoplasmic organelles, that are the principal sites of ATP synthesis; they also contain enzymes of the citric acid cycle and for fatty acid oxidation, oxidative phosphorylation, and other biochemical pathways. (fig.2)
The electrons from oxidation of NADH and FADH2 are not directly transfered to oxygen, but pass 3 protein - complexes with increasing affinity to electrons. They are NADH - coenzyme - Q - reductase (succinate - coenzyme - Q - reductase for FADH2), coenzyme - Q - cytochrome - c - reductase and cytochrome - c - oxidase, that are build from cytochromes, flavoproteins and ferric - sulphur - clustern (fig.2).

Fig.2: Mitochondrial electron transport. The electrons are transfered via the coenzyme Q from complex I to complex III and via cytochrome - c from complex III to complex IV
In an alternating process of oxidation and reduction the electrons are transfered from one complex to the other and finally they are transfered to O2. Per electron, which passes this transport system, there are 3 protons carried from the matrix to the space between the membranes, which leads to a membrane potential resp. to a pH gradient that stimulates the ATP synthesis. With the gain of energy from the return of approximately 3 protons to the matrix, one ATP molecule can be produced because of phosporylation of an ADP molecule with Pi (fig.3)

Fig.3: Linkage of the electron transport and of the ATP synthesis by producing an electrochemical gradient of protons by the inner mitochondria membrane. During the transport of electrons H+ is pumped out of the matrix, its return powers the ATP synthesis.
Normally these processes also go on in the dark and in each sound cell. If such cells additionally are irradiated with light, the enzyme complexes are supported in their redox - process by the so-called photo oxidation. Photooxidation is a process, in which light stimulates a donor molecule to hand over an electron to an acceptor and itself is oxidated, while the acceptor is reduced. This process works, because electrons in their stimulated state are less bound to the molecule than in their basic state. The energy of absorbed photons is chemical transfered to the redox centres of the enzyme complexes of the respiratory chain, and therefore they are more easy oxidated resp. ionized and the ATP synthesis is increased. Here the key function of this the light - metabolism - interaction shall be mentioned again. The idea of oxidation in chemistry, that is the release of electrons, is the same as ionization in physics, an atom or molecule looses an electron. It is commonly known, that ionization is more likely from a stimulated (by light) energy level.
The dependence of light stimulated ATP synthesis from the wave lenghth of the radiated light is determined by the absorption properties (which slightly change in oxidated resp. reduced state) of the single components, the enzyme complexes, mainly of the cytochromes.
T. Karu recorded e.g. the action spectrum of DNA synthesis of exponential growing HeLa - cells during the irradiation in the range of visible wave lenghth. (Fig. 4)

Fig. 4: Action spectrum of the DNA-synthesis rate of exponential growing HeLa cells at visible monochromatic radiation (energy density 10 J/m² and 100 J/m²) measured 90 minutes after irradiation
The data show, that there are 2 groups of spectral sensitive ranges. One covers the nearby ultraviolett and visible blue wave lenghths of about 350 - 450 nm, the other covers the range of the visible red and nearby infrared wavelenghth of about 600 - 830 nm. A lot of such experiments with prokaryotic and eucaryotic cells let T. Karu show, that light receptors in blue wave lenghths are flavoproteins (fig. 5) of the reductases (dehydrogenases) and in the red wave lenghths the semichinon type of the flavoproteins of the reductases (dehydrogenases) and the cytochrom a/a3 (fig 6) of cytochrom - c - oxidase. Such studies are easy because of the principle of photochemistry, an action spectrum always reflects the course of the absorptionspectrum of the light absorbing molecule.
Such studies in context with clinical experiences have shown, that for maximum stimulation, not only energy densitiy have to lie in a certain range, but also the output densitiy and therefore the time of irradiation. Especially interesting is, that the specified optimal parameters for irridiation correspond very well with clinical experiences.
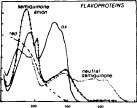
Fig. 5: Absorption spectrum of Flavoproteins

Fig. 6: Absorption spectrum of Cytochrome a/a3
Why does the stimulation of the respiratory chain result in an increased proliferation of cells?
The answer is simple: Light induced increasing of ATP
synthesis and building of a proton gradient lead to an increasing activity of
Na+/H+- and Ca2+/Na+- Antiporter
and of all ATP- driven carrier for ions, such as e.g. Na+/K+-ATPase
and Ca2+- Pumps. ATP is the substratum for adenyl cyclase, and
therefore the ATP level controls the level of cAMP. Both Ca2+- and
cAMP - level stimulate the synthesis of DNA- and RNA, which leads to an
increased cell proliferation. Fig. 7 shows this so-called "light - signal
- transfer - chain", first described by
T. Karu.
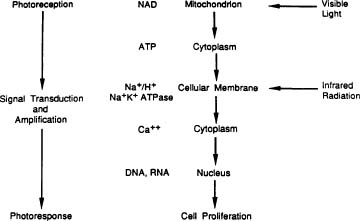
Fig. 7: Light signal transfer chain, set up by T. Karu and changed by K.C.Smith
Please notice, that cAMP and Ca2+ are very important second messengers. Especially Ca 2+ regulates almost every process in the human body (muscle contraction, blood coagulation, signal transfer in nervs, gene expression, etc.)
From the view of an user of low level laser therapy (LLLT) the question arises, what is the "right" or optimal wave lenghth. Though the results in fig 4 show, that stimulation results are the same in the near UV- and blue- range as in the red or infrared range, but with a tenth of the energy density, it is better to use a redlight laser. The reason for this is, one have to consider the depth of penetration into the body, which depends highly on the wave lenghth. Mainly there are two layers: the skin and the tissue. While infrared penetrates the skin better, penetration depth of visible red light in living human tissue is a bit higher (fig. 8)
Fig. 8 shows clearly, that maximum transmission lies by approximately 700 nm. In the blue range transmission is 50 times lower. (O.D. means optical density, large O.D. - little transmission, and vice versa) The use of wave length in the blue range makes sense only for superficial applications.
Since wave lengths from 670 to 690 nm support the redox processes of some intermediate steps of the respiratory chain, modern therapeutic lasers shall provided with these wave lenghths. Now, after six years of clinical experiences of about 1000 therapeuts, it is evident, that these wave lenghths show better results than He-Ne-lasers (632,8 nm)
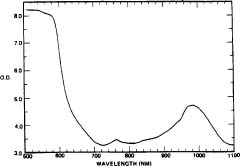
Fig 8: Absorption spectrum of a living human hand
Since there are enough studies, which confirm, that one could have therapy success with infrared lasers (750 - 1000 nm) (though clearly poor ones), the question of infrared mechanism comes up. K.C. Smith tried in one of his publications to give an explanation. He states, visible radiation causes photochemical alteration (stimulation of the respiratory chain) because of its higher quantum energy, while infrared radiation causes photophysical effects, such as rotation of molecules and vibrations, that effect cell membrane. Therefore he completed the photo signal transfer chain, suggested by T.Karu in a way, that IR radiation influences the metabolism cascade via photophysical effects at the membranes, possible at the Ca2+ channels. (fig. 7). Though this is a very plausible explanation, it is unlikely, that there is an exact border between the mechanisms in visible and infrared spectral range. Fig 6 shows that is possible to stimulate directly the cytochrome a/a3, even though less strong. This is also shown by the above mentioned clinical results: With increasing wave lenghth stimulation results decrease resp. the required power and energy density increase.
Another question would be, how far physical alterations in the cell membrane could have the typical regulative character for LLLT, as they have with stimulating the respiratory chain. This field has to be examined thoroughly!
Stimulation of Immune response
Another important effect of LLLT is the stimulation resp. the regulation of immune response. It was one more time T.Karu, who discovered, that laser radiation in- or decreases the production of oxygen radicals such as superoxide - anion O2.-, hydrogen peroxide H2O2, hydroxyl- radical HO. and singulett- oxygen1O2. These studies were carried out with cultures of mouse - splenocytes - suspensions and the amount of oxygen radicals was measured by chemiluminiscence. Again it was shown, that LLLT is a regulation therapy. Depending on the composition of the splenocyte - suspension, the production of the radicals was in - or decreased. While the formation of radicals increases with the number of plasma cells, neutrophil granulocytes, myelocytes and metamyelocytes, a large number of lymphocytes decreases the amount of radicals. (fig. 9, 10) As the compostion of cells changes with the pathological status of the body, it is clear, how the laser radiation can regulate the immune response.
There exist two possibilities for the development of oxygen radicals and therefore for the location of the stimulation: The phagocytosis induced NADPH-Burst (respiratoric burst), which build up from the activating of the NADPH-Oxidase-Systems in macrophages or neutrophil granulocytes, and the development of radicals in the oxidative metabolism (respiratory chain). In the first case the semichinon type of flavoproteins is the possible receptor for light, in the latter it is cytochrome a/a3.
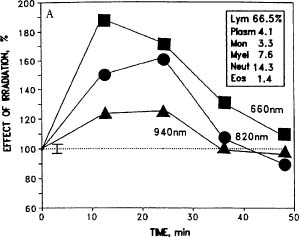
Fig. 9: Increasing of the radical production
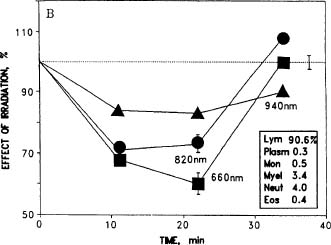
Fig. 10: Decreasing of the radical production
Reduktion der Radikalbildung
Since laser radiation increased production of radicals is approximately one order smaller than the one that is induced by phagocytosis defending microorganism, one assumes, that radicals develop in the latter part of the respiratory chain. It shall be noticed here, that the examination of radical development in medicine is just in its beginning. Radicals can not be measured directly, one have to make the detour via chemiluminiscence.
Radicals, that develop in each sort of metabolic activity, are not bad for the organism in the first place. Developing and destroying have to be balanced. H2O2 is a necessary substrate for peroxidases, which take an important role in detoxicating the organism. If all H2O2 in peroxisomes would be neutralized by catalase to H2O, an important protection mechanism would be lost. Again it is clear, how and when, laser radiation is able to regulate.
Looking at fig. 9 and fig. 10, which show the stimulation resp. the rduction of radical development depending on the time after the irradiation and on the wave lenghth, one notices, that stimulation as well as reduction of the radical production is strongest within the range of visible wave lenghth. Effects are weaker by increased wave lenghth. The same study shows, that the effects of LLLT depend on the energy density and stimulation resp. reduction decrease with higher frequency. It is also shown, that coherence of radiation is not demanded: The wave lenghth of 660 nm was developed by a super bright diode and not a laser!
In the meantime studies exist about ultra structural alterations in human lymphocytes during irradiation with He-Ne-laser.
The analgetic effect
The analgetic effect of LLLT is clinical very impressive. Just think about the loosen tension - feeling after one minute in herpes labialis or in an onsetting otitis media in children. Mechanisms are very complicated: E.L. Laakso was able to confirm former examinations in a study about laser - induced analgesy in different orthopedic disorders accompanyied by chronical pain, in which laser radiation leads to degranulation of mast cells and release of inflammatory mediators and lymphocines out of macrophages. Lymphokine Interleukin-1 activates via the release of Corticotropinreleasinghormon (CRH) from the Hypothalamus the pituitary - adrenal - axis. CRH comes through portal vessels to the anterior lobe of the potuitary gland and causes in POMV cells the release of the cleavage products of the precursor - polypeptide - proopiomelanocortin (POMC) that is the adrenocorticotropin (ACTH), also known as corticotropin and the release of b - endorphines. While b - endorphines lead to an opioid receptor resp. light mediated analgesy, ACTH reaches via the common bloodcircle the adrenal cortex, where cortison (and other glucocorticoids) is released, and such effects immune suppression and inflammatory inhibition. At the same time a feedback inhibition of CRH release in the hypothalamus occurs. Additionally cortison gives a negative feedback on the CRH and ACTH release. And therefore laser interferes with a control system again.
As the patients were irradiated at triggerpoints, it was proven, that a peripheral stimulus with laser leads to a stimulation of the CNS and the immune system. Laakso also cites a study, that supposes the existence of a local CRH system. Therefore LLLT as one more time not only a local, but also a systemetical effect. A property, which sadly is overlooked from time to time in "left - right - comparising" - studies and as such lead to "insignificant" results of LLLT.
Another study on the effect of LLLT in different chronical pain symptoms was carried out by J.B. Walker. He showed, that irradiation with a He - Le - Laser leads to a rise of 5 - hydroxyindol acetic acid, a decompositon product of the neurotransmitter serotonin, which occurs in urine a few days before soothing of pain sets in.
The impressive results, especially in chronic pain, may be closely connected with the cabability of nerve cells for learning and memory. According to lastest knowledge nerve cells respond to long lasting and repeated stimulus with overreacting resp. spontanous activity. The ability for memory come about the fact, that (transmitting the stimulus at synapsis) released neurotransmitters l - glutamat and substance P set on the production of second messengers in nerve cells such as CAMP and CA2+, which on their part increase the gene expression of stimulant transmitters and the pertaining membrane receptors.
"Forgetting" these traumatic "information" demands an increased expression of inhibitory receptor genes resp. reduced expression of exitatory receptor genes. This process takes more time, the longer the nerve cell has been in this hypersensible state.
As mentioned above, the light induced increase in ATP synthesis through light signal transfer chain (fig 7), causes a boost of gene expression. If the inhibitory transfer systems are concerned, the function of a laser induced analgesy is clear.
The "process of forgetting", that is learning the pain free status, is also supported by the other effects of low level lased radiation.
Soothening of pain is also caused by other effects of LLLT: Edemas, which occur with each tissue damage, produce pressure on the adjacent sensoric nerve ends, which again lead to strong pain. The strong anti edematous effect of the laser leads to a quick reduction of pain and the "process of forgetting" may start.
Summary
If one stays within the range of the specified output density of 1 - 100 mW/cm², for which the producers have to guarantee, the clinician is provided by the regulating character of LLLT with an absolutely side effect free therapy method. Therefore it is no problem to start, it even is fun, for the patient too (children!), because LLLT is non invasive. Besides the direct irradiation of the retina (which is prevented by the eye through the palpebral closing reflex when irradiated with visible wave lenghths), there are no contraindications. The doctor is again able to "test" with good conscience new therapy concepts. Maybe it is important to handle laser beams as carefull as medicaments: Tolerance effects are not described in literature, but otherwise they are not to be excluded. Therefore: Always start with lowest doses, the dose could be increased during the therapy.
To observe and to feel is the most important with regulation therapy, because despite the good research on basics it is not known, how many photons are required. A laser with an output of only 1 mW and l = 670 nm issues after all 3.1015 photonen /sec.
All therapeuts, who want to treat injuries without antibiotics, can count on the fact, that laser beams stimulate the production of oxygen radicals for immune response.